Population Health
Our work with populations in York goes beyond diagnosing and treating illness, putting more emphasis on improving well-being and preventing ill health.
Improving Population Health
One of the biggest challenges facing health and care in our area is the growth in the number of people living with long-term conditions such as kidney disease, asthma or diabetes. Many of these conditions can be prevented, and even after diagnosis the onset of more serious symptoms can be delayed through a preventive approach. Over the last decade, there has been an increase in the number of patients on primary care disease registers in the Vale of York.
Population health approaches recognise that the NHS cannot simply organise its way out of these trends through greater efficiency, and must therefore work with partners such as Local Authority Public Health teams on the wider social and behavioural factors which keep people well or support them with their conditions beyond the hospital or surgery door.
One way we have been doing this in the Vale of York is through a tool known as Population Health Management (PHM). This applies public health expertise to routine health datasets to understand current and future health and care needs, so action can be taken to design proactive models of care. The box below defines the difference between wider ‘population health’ and the narrower ‘population health management’ tool:
| Population Health is an approach aimed at improving the health of an entire population. It is about improving the physical and mental health outcomes and wellbeing of people, whilst reducing health inequalities within and across a defined population. It includes action to reduce the occurrence of ill-health, including addressing wider determinants of health, and requires working with communities and partners Population Health Management improves population health by data driven planning and delivery of care to achieve maximum impact. It includes segmentation, stratification and impactabilty modelling to identify local ‘at risk’ cohorts – and, in turn, designing and targeting interventions to prevent ill-health and to improve care and support for people with ongoing health conditions and reducing unwarranted variations in outcomes. (NHSEI PHM Flatpack) |
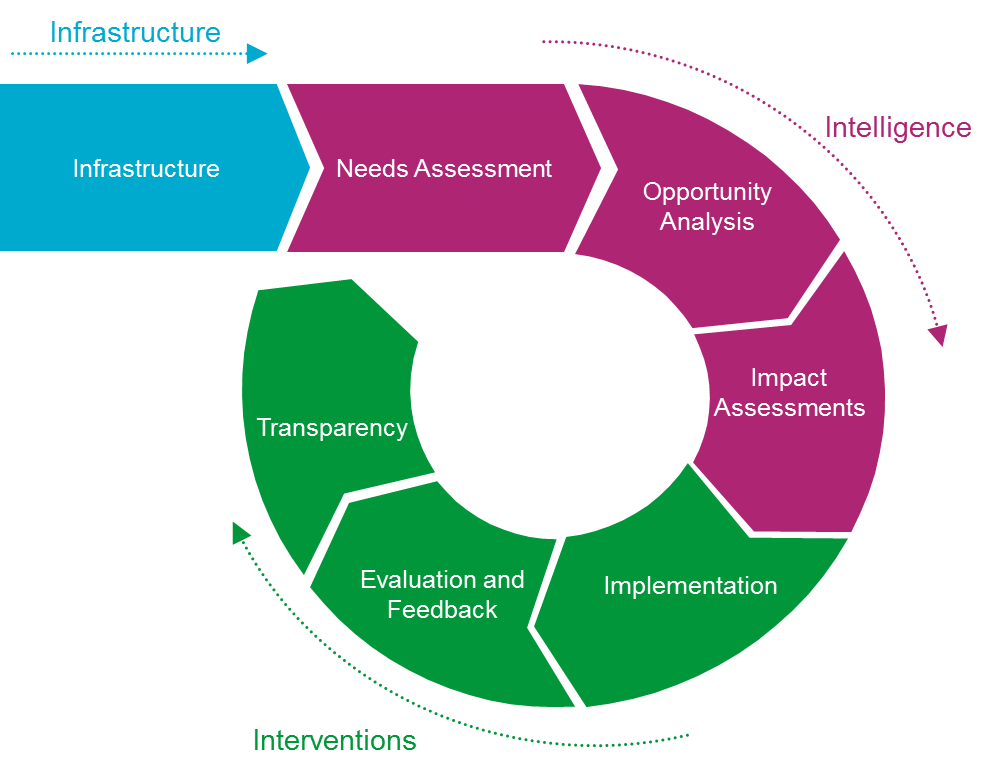
PHM is, in essence, a ‘quality improvement cycle’ applied to whole populations rather than individuals. It needs 3 capabilities: the right infrastructure to bring together linked data on populations across primary, secondary, and social care; the right intelligence to understand what the data is telling us; and the evidence-based interventions which are implemented and evaluated. This is shown in the diagram below:
Click on the following links to find tangible examples of this work in York:
- City of York